I’ve been thinking about that a lot lately. I’ve been reading Wil Wheaton‘s book “Still just a geek”. It has reminded me to write more regularly, but it has also encouraged me to work more on my next books (I have two in the works). His writing encouraged me because I’m sure I can write just as well. Now I don’t have any “celebrity” so I don’t think my books will sell much – I definitely need to do more ‘marketing’ of my book. Now that it is available on a website that isn’t Amazon, I could choose to buy some Google Ads for the book. I would be very specific and use the search words “breast cancer” and “memoir” such that the person who typed those two words would learn about my book – that would really help increase sales.
Anyways, I’ve decided to spend more time writing. I will make an effort to spend at least one hour per day writing. This won’t necessarily be something that I share – in that I might just write in one of my personal journals.
Other than the book, what else has my inspired to write is a workshop I’m attending put on my April Stearns of Wildfire magazine. I attended the first workshop yesterday. It really helped me get back into writing and some of her prompts have given me an anchor point onto the page. It also felt a little like one of the support groups I’ve been craving. Since Wildfire is about the experiences of those who were diagnosed young, it would make sense that sharing time and stories with this group would feel like a support group. It is exactly what I need right now, as it is helping me move forward with writing practices.
One of the prompts was “what I expected? what I got?” That brought out a interesting series of questions that I was asking myself.
I expected that I had already gone through my ‘mid life crisis’, and yet I find myself needing to reinvent myself yet again. Who am I after this cancer experience? How do I bounce back from it? What are the essences of my life? What is my legacy? and why do I care about legacy?
I find it interesting that I was thinking about legacy – and it brings up the question “why do I care about legacy”. In some ways, legacy helps with the idea of not living a long life, because then something of me will be living on. The world that remains will see my ‘footprints’ in my blogs, my podcast, and my books – oh ya, and my Masters Thesis and various obscure academic publications.
My legacy will be of someone who:
helped to build Treehouse Village (although I think that is really more of Scott’s legacy)
wrote a book or two about her breast cancer experience
wrote a book or two about her 16-month bike trip around the world without airplanes
wrote a textbook or two or three or more about instructional design
I hope that I will also be remembered as a kind, generous, and thoughtful person.
I then ask myself, what parts of my legacy need work? What other things do I need to achieve to make my life feed complete?
I’m definitely having a “mid-life crisis” (or “later-in-life crisis”). I am feeling that I will need to rebuild myself again, and I’m not sure what I want that ‘new me’ to be.
In the fall I will go back to work. I’ll actually start working in August, as I have a lot of prep work to do for the two courses I’m teaching. I know from experience that there isn’t a lot of use in doing it too early – as I will forget what I decided to do – so better to be teaching closer to the time I made the decisions.
I guess that is another part of my legacy – all the students that I have taught and who remember me as someone that pushed them to learn, and helped them realize that they can do more than they thought. I continue to keep working at uMass because I love teaching and I love teaching the students in the instructional design program. Imagine small classes where everyone is there because they want to be and they are eager to learn new things. Yup, that is why I love my current job.
One of the things I know I want to be in my legacy is the work that I have done and do in writing. That encourages me to get back to finishing a couple of books. The Going East book is particularly interesting one, and one that I had regretted not doing when I had my first cancer diagnosis. I’ve done more work on it. I’m putting it all together and hopefully someday before I die, I publish the book(s). I cannot get it into a single book, there is just too much write about – too many stories. I just need to figure out what reasonable sized books are, and then where there are logical places to break things up.
So, I guess, I want the biggest part of my legacy to be about me as an author, which means I need to do a lot more writing!
This post is a continuation on my discussion about Patient Health Literacy. The narrative that resulted from this study has been published on Amazon. See my Memoir page. The original source that I used for my study can be found at https://bcbecky.com.
In reviewing the posts categorized as Navigating the healthcare system, I constructed the following themes: (1) learning processes, (2) taking control, (3) dealing with insurance, and (4) waiting. The theme learning processes applies to posts where I describe the different interactions I’m having with healthcare providers. The theme taking control applies to posts where I voice my need to empower myself or others by exerting some form of control over a situation. The theme dealing with insurance applies to posts where I write about issues insurance coverage of medication and treatments. The theme waiting applies to posts where I write about issues with waiting for various test results or treatments. I discuss each of these themes in more detail in the in the following sections.
Learning Processes
In the beginning I had no understanding of how the medical system worked with respect to cancer treatment. My understanding came only from what I saw on television and from an acquaintance that I sailed with 15 years ago who happened to be a medical oncologist. From that, I knew that there were different types of oncologist, but I did not understand that breast cancer treatment typically begins with surgery. Throughout the blog, I explore and share my interactions with the medical system, as I learn to negotiate it.
In Canada, I likely would not have had much choice in where I received treatment. I also would not have thought that a I had any choice in surgeon or oncologist. I would go to who I was referred to. In the US, and specifically in the area where I live, there are multiple providers. In some ways insurance affects where you get treatment, but I had really good insurance that allowed me the option of choosing. After hearing the words ‘you have cancer’ I felt an immediate sense of lack of control. The ability to choose a healthcare provider, although stressful and a completely new process for me, was also a way to exert some control over the situation.
As all the processes were new to me, I explained them in detail as they occurred. For example, in A long day (June 19, 2014), I explain the process of the appointment with the surgeon as well as the “whirs, honks, and other sounds” associated with my first experience with magnetic resonance imaging (MRI). I continue with the description of processes on my first day of chemotherapy, where I also include images that provide visual documentation of the process (First day of chemo, July 7, 2014). Further, in This too shall pass (July 16, 2014), I describe how:
They don’t give you much other than anti-nausea meds for the first cycle, and they wait for you to call. The idea is that everyone experiences chemo differently, so they don’t know what you will need. They wait until they find out what you need then prescribe it. At this point, it is all about managing the symptoms. Unless the problem is life threatening (more life threatening than the cancer), the goal is to keep with the chemo regime on schedule through to the end.
In addition to describing the medical process, I also described what I learned about the process of gathering information from my care team. In I had to give myself permission to nap (July 9, 2014), I outline what I learned about how nurses and physicians provide different levels of information:
Nurses tend to provide advice on the extreme side of things. For example, absolutely no alcohol, no swimming, no biking. They tend to provide advice based upon the worst-case scenario, but also discount mental health. The need to exercise is important to my mental health. The oncologist is good – he explains the chemo cycle – and says it is OK to swim the first week, but as my white blood counts get low to stop swimming until the counts return.
My analysis also shows that, in addition to describing the processes as I recalled them, I also wrote about my observations regarding medical education from the interpersonal perspective:
What has been interesting is that this seems to be part of the learning process. Those who are most empathetic are the attending surgeons. The residents are still learning, so their interactions can feel a little mechanical – they are still trying to figure out the best ways to make connections with patients, but also the best ways to describe things. By the time they are fellows, you see a higher level of confidence in their ability to provide patient education – and you start to see information that is more customization to your specific case. The attending surgeons seem to be the best at tailoring their discussions to your specific situation.
Finally, when I was hospitalized after surgery, I described my experience with hospital processes, specifically how a private room meant that my husband could stay the night with me, and the quality and process of getting food: “One thing that impressed me about the university hospital is that they use a room service model for food. The menu is quite good, and so far, the food has been good. The food is locally sourced where possible, and there are organic options” (An update from the hospital, November 20, 2014).
Taking Control
From the beginning I tried to take control by booking appointments for a second opinion from the university healthcare system. Here I was immediately frustrated at an inability to get an appointment without a confirmed pathology. Fortunately, they did guarantee me an appointment when the pathology results were confirmed (The speed of things, June 15, 2014). After getting an appointment, the act itself of seeking a second opinion and making a choice as to where to get healthcare were ways that I could take control (Double-mastectomy and chemo, June 19, 2014).
When I began to experience some odd side effects, specifically blisters on my hands, that were not resolving, we made the decision to go to the emergency room. This was in part so that we could experience the process of the emergency room at a time when we were not overly stressed – that is, “while I was happily ambulatory and not ‘really sick’, just in case I needed the services at a later time” (Not without incident, July 13, 2014). Further, in Engaged patient in a hospital gown? (September 27, 2014), I describe the process of a typical doctors’ appointment – and how I take as much control as I can during those appointments, in this case by wearing a hoody over the hospital gown.
Dealing with Insurance
The role of insurance in the treatment for breast cancer both surprised and outraged me. I was surprised when one of the first things the surgeon told me, after telling me he recommended a double mastectomy, was the ‘good news’ that insurance was required to pay for reconstruction (How do you prepare to lose a body part?, June 15, 2014). I was surprised when the oncologist mentioned that “it also takes about a week to get approvals from the insurance company” (Caution – this one talks a bit about death, June 21, 2014) before I could start chemotherapy.
We ran into issues with insurance and treatment after my first day of chemotherapy, which required the white blood cell booster Neulasta to be administered the following day. Insurance changed the way in which it was to be delivered (Pains with the American System, July 7, 2014). Finally, with a slightly more nuanced understanding of the way insurance impacts healthcare in the United States, I write a response to a New York Times article expressing my concern “that research stated like this gives insurance companies a reason not to pay for the surgery, when it may be in the best interest of the individual” (Bilateral mastectomies, July 28, 2014).
Waiting
Waiting was something that I ran into from the very beginning. First it was waiting for the pathology results, as I could not make an appointment at the university cancer center without confirmed pathology (The speed of things, June 16, 2013). When we were deciding on where to get treatment, we knew that we would be spending more time waiting at the university cancer center. We took waiting into consideration when making our decision, specifically I write:
In the first couple weeks after diagnosis, I had decided where I was going to get treatment. I based this, in part, on where I felt comfortable – but also who provided me with the most options. I really liked being in a teaching setting and having access to more specialists – but that was balanced with knowing that I would spend more time in waiting rooms and receive less fancy care (e.g. the infusion treatment center doesn’t provide lunch).
As I went through treatment, there were many occasions where I describe what I felt to be excessive wait times. For example, “It turned into a long day. We had a delay seeing the nurse practitioner to get sign off on chemo – unfortunately that turned into a three-hour delay. Then we had a delay on the saline drip for rehydration, which added another additional hour” (AC Cycle 4, August 19, 2014).
As we became more familiar with processes, we became more efficient with our time, developing strategies to reduce the amount of time we spent waiting. When I became more confident in myself as a patient advocate, I learned to identify problems in the system and articulate them to management in hopes of resolving the issue. For example, in Learning to assert myself, (October 29, 2014), I write:
Today, I asked for a supervisor. You see, I had an appointment. The online system showed my appointment as 9:15. I was told to arrive 30-minutes prior to my appointment (which is a bit excessive). I arrived 25-minute prior to my appointment (8:50). When I was still waiting at 9:30, I went to talk to the receptionist. Anytime I’m asked to wait more than 15-minutes, I want to know why I’m waiting (that is a lesson I have learned here – in Canada I would just wait in silence – it is interesting how asking goes against my ingrained behaviour). I found out that my actual appointment was at 9:45. The online system had already added 30-minutes, and the person who made the appointment for me added another 30-minutes. This is in part why patients spend excessive amounts of time waiting.
Summary
Nursing research shows that supporting breast cancer patients with navigating the healthcare system can improve many aspects of the care that patients receive (Robinson-White, Conroy, Slavish, & Rosenzweig, 2010). My analysis of the category Navigating the healthcare system shows that I had regular interactions with the healthcare system, and there were spikes in my interactions associated with receiving pathology results, starting chemotherapy, exploring surgery options, and surgery itself. Under the category Navigating the healthcare system, I constructed the following four themes: (1) learning processes, (2) taking control, (3) dealing with insurance, and (4) waiting. As I learned the processes associated with receiving cancer care, I wrote about them. When I was able to, I sought ways that I could take control over my interactions with the healthcare system. Unfortunately, there were two areas of challenge with my experience with the healthcare system, dealing with insurance and what felt like unnecessary waiting.
Each person experiences breast cancer differently. This difference is in part related to the variable nature of the disease, but also the different healthcare systems where the patient is seeking treatment. The nursing profession has attempted to address this complexity with the creation of formal nurse navigators that help guide cancer patients through the healthcare system (Case, 2011). Unfortunately, not all healthcare systems have nurse navigators. In addition, the nurse navigators are often not fellow breast cancer survivors. This means that they cannot fully appreciate what it means to live with the illnesses associated with breast cancer and its treatments. The nurses are also insiders within the system, with knowledge and privileges that patients do not have. This can lead to a gap in what information the patient needs. Patients experiencing critical or chronic illness have a need to learn how to navigate the healthcare system from a patient perspective.
This post is a continuation on my discussion about Patient Health Literacy. The narrative that resulted from this study has been published on Amazon. See my Memoir page. The original source that I used for my study can be found at https://bcbecky.com.
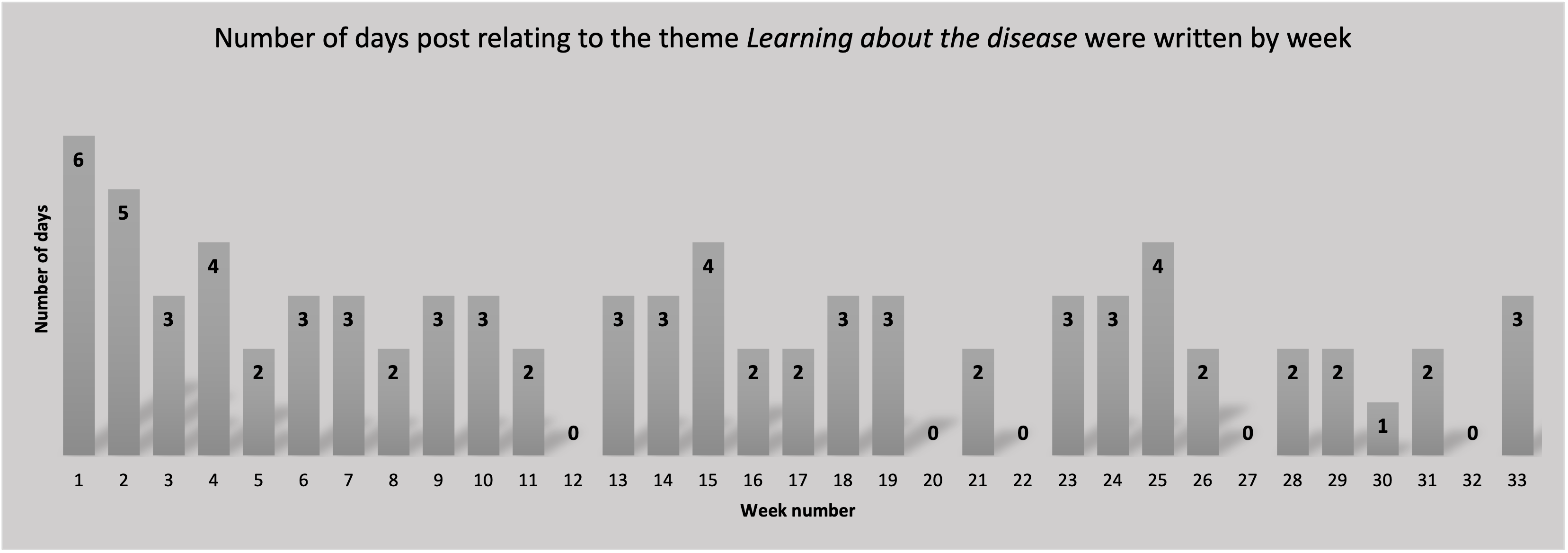
From among the 237 blog posts, I coded 92/237 (38.8%) with the category, Learning about the disease. The distribution of number of days per week that I wrote one or more posts that were coded as Learning about the disease, Figure 4, shows interactions almost every week. This is particularly interesting because it shows that the learning did not just happen at diagnosis, rather I continued to learn and share my learnings throughout the study period.
Number of days per week that a post was written that has been categorized as Learning about the disease.
In reviewing the posts categorized as Learning about the disease, I constructed the following themes: (1) sourcing experts, (2) sourcing the Internet, (3) sourcing academic articles, and (4) sourcing peers. The theme sourcing experts applies to posts where I echo the information I receive from healthcare providers. The theme sourcing the Internet applies to posts where I include information from trusted Internet sources. The theme sourcing academic articles applies to posts where I include references to academic literature. The theme sourcing peers applies to posts where I describe information that I have gathered from peers such as through support group meetings. Peer sources includes blog posts of other cancer survivors. I discussion each of these themes in more detail in the in the following sections.
Sourcing experts
When I was initially diagnosed, I knew very little about breast cancer. In my early posts I would parrot back of the words I heard from my healthcare providers. For example, in It all started… (June 14, 2014) I say, “I’ve been told that the majority of women who get breast cancer do not have relatives with cancer”. As I gather more specific information, I include my interpretation and feelings associated with the information I’m receiving. For example, in Double-Mastectomy and chemo (June 19, 2014), I write not just about the disease characteristics, but also what those characteristics mean and how that translates into a treatment plan. At this point, I am echoing the information the I received from an oncologist. I’m not referencing any other source. More importantly, in this post I’m not just talking about the data itself (that is the pathology), I’m also talking about what that data means and how that information affects the recommended treatment options.
Sourcing the Internet
Within support groups, I often heard the women say to someone who is newly diagnosed ‘do not look at the Internet’. And yet, it was the Internet that I went to when I needed to look up medical terminology. When interpreting my pathology report, I tell readers of my blog that if they want more information on how to understand pathology reports, to look at http://breastcander.org. I refer to this site several times within the blog, as it provided useful information regarding breast cancer and treatment options.
When I wanted a description of medical terms, or when I wanted to validate something that I heard from either support groups or healthcare providers, I went to trusted sites on the Internet. In Significance of dates and getting ready for chemo (June 26, 2014), I write about my reflections on the chemotherapy preparation class that my husband and I attended. I share a couple of resources: a book that I found to be not very useful; and, a website, http://chemocare.com, that was very useful. I find it particularly interesting that advice is often given to ‘not look at the internet’, and yet the better and more current resources shared are those found on websites rather than books, which quickly become outdated.
Sourcing academic articles
Initially, I was unable to read academic sources, rather, I relied on my husband to do that research. However, when I had to make a decision regarding surgery, I reached into the academic literature to do an analysis on what the surgery and the expected results of neoadjuvant chemotherapy. For example, in Breast reconstruction – academic analysis (September 22, 2014), I write about the knowledge I gained through reading academic articles relating to the type of breast reconstruction surgery I was debating. In addition to sharing some of the key findings from the academic articles, I also shared terminology definitions such as “Autologous reconstruction is reconstruction that involves the patient’s own tissue (e.g. DIEP flap, TRAM flap).” In Pathological Complete Response (September 23, 2014), I write about the knowledge I gained, and my interpretation of academic articles associated with the expected outcomes of neo-adjuvant chemotherapy. I not only provide key findings, but I provide my commentary on the findings. I’m sharing both the findings from the articles and my interpretation of that information and how it applies to my situation.
Sourcing peers
In addition to healthcare providers, friends connected me to a fellow breast cancer survivor. I see echoes of conversations I had with here in my blog, for example when I say “choose who you want to trust, and then trust them” (A long day, June 19, 2014). By the time I was to start treatment, I was familiar with some of the expectations around treatment. For example, in This too shall pass (July 16, 2014), I say that “during support group last Saturday, one of the ladies explained what the Neulasta bone point felt like. I had been warned.”
Perhaps the biggest benefit from support groups was the normalization of medical terminology and the generic breast cancer treatment process. Specifically, in A photo shoot and getting ready for surgery (November 18, 2014), I write about the process of the surgery. I specifically talk about the “injection of some nuclear isotope into each breast that helps to identify the sentinel node, and the insertion of wires to guide the surgeon to the exact location of each of the tumors”. By the time I wrote about the procedure, the concepts had been ‘normalized’ for me. I had heard about it so many times at support group that I came to think of the process as ‘normal’. It was just something that I needed to do. Further, in Breast reconstruction – Academic analysis (September 22, 2014), I point to another blogger’s post before I refer to the academic literature: “First off, I should start by pointing out an important blog post written by Nancy Stordahl on why breast reconstruction is not a boob job (2013). When looking at patient satisfaction, I focused on post-cancer reconstruction which is a lot more complex than cosmetic reconstruction.”
I don’t share a lot of the medical information that I received in support group. In part because I often validated this information with my healthcare provider and then reported it in my blog as being from my healthcare provider. In Flyin’ (November 26, 2014), I write about information that I learned from various support groups pertaining to lymphedema, and then how I looked into the academic research about it, sharing some key points from the research. Here I am showing how the information I received through support group helps me know what to look up, but also how I do not directly trust the information in support group, rather I look to more trustworthy sources.
Summary
In order for patients to be partners with their healthcare team in making appropriate decisions, patients need disease-specific information (Wallberg et al., 2000). When I was diagnosed, I knew almost nothing about breast cancer. I needed to use multiple sources in order to learn about the disease. My analysis of the category Learning about the disease shows that I continued to learn about the disease throughout the treatment process. Under the category of Learning about the disease, I constructed the following four themes (1) sourcing experts, (2) sourcing the Internet, (3) sourcing academic articles, and (4) sourcing peers. Within these information sources, I did not only share the information directly, I also shared the way in which I was interpreting the information. In addition, as time progressed, I increased where I received my information, using multiple sources to validate what I was learning.
I began my learning about breast cancer through information I received directly from expert sources, that is my healthcare providers. When I needed clarification on terminology or more detailed medical information, I sought out trusted Internet sources. When I was ready to read academic literature, I searched the literature for information that would help me make treatment decisions. The different information and advice sources sometimes overlapped, where at other times they didn’t. I had to learn how to discern not only where I could get information, but also what types of information I could get from where, and how reliable that information was. There were so many nuances to information that I didn’t always appreciate at the time, and some that I still don’t appreciate. Throughout the process I negotiated the information that I received from expert sources, Internet sources, and academic sources. Although I gathered information from peer sources, I did not directly trust that information, rather I used trusted sources to validate what I had learned through peer sources. Patients experiencing critical or chronic illness have a need to learn appropriate sources for different types of information to help them learn about the disease and what it means to live with the disease.
Where do you find your health information? What sources do you find reliable? Where do you learn about how to live with the disease?
This post is a continuation on my discussion about Patient Health Literacy. The narrative that resulted from this study has been published on Amazon. See my Memoir page. The original source that I used for my study can be found at https://bcbecky.com.
From among the 237 blog posts, I coded 163 (68.8%) with the category, Developing coping mechanisms. The distribution of the number of days per week that I wrote one or more posts that were coded as Developing coping mechanisms, Figure 2, shows that from the very beginning and throughout treatment I blogged about coping mechanisms. There are dips that align with the weeks where I wrote fewer posts overall and can be attributed to times where I was travelling or having surgery.
Figure 2: Number of days per week that a post was written that has been categorized as Developing coping mechanisms.
In reviewing the posts categorized as Developing coping mechanisms, I constructed the following themes: (1) blogging, (2) exercising, (3) social networking, and (4) seeking control. The theme blogging applies to posts where I write about or reflect upon the act of blogging. The theme exercising applies to posts where I write about exercising including hiking and being in nature. The theme social networking applies to posts where I write about connections with others that provide me support. The theme seeking control applies to posts where I am writing about ways that I try to find aspects of disease experience where I can create a sense of control. I discuss these themes in more details in the following sections.
Blogging
In the beginning, I highlight that I began blogging as a way to share my thoughts, as I was a blogger before diagnosis, I found myself wanting to write and share my experiences as a way to process what was happening to me, specifically I say “I shall look at this blog as a journal into lived experience, combining medical jargon with lived-experience of someone with breast cancer” (It all started …, June 14, 2014). A few days after diagnosis, I discovered another benefit to blogging, specifically that I didn’t have to keep telling people what was going on. I wrote “Mostly I’m pointing people to my blog, just so I don’t have to keep saying it. There is an emotional toll that occurs on both sides. Some people want to reach out and talk, but I’m not there yet. I cannot talk about it.” (A tough day, June 17, 2014). Later, I write about my intention to use my blog as a way to exercise my brain when I was worried about the effects of chemotherapy on my cognitive function. I wrote: “I shall keep up my ‘exercise’ and try to write regularly. I can only hope that my words continue to make sense and continue to demonstrate some level of cognitive competence” (Reflection on chemo brain, September 15, 2014).
I talk explicitly about the blogging process at the beginning of the treatment process, but then stop writing about the blogging process as treatment progressed. This suggests that my reflections on blogging itself became normalized as treatment progressed, that is, that I no longer felt it necessary to reflect on how blogging was affecting me.
Exercising
From the beginning, I recognized exercise as a priority, noting that I wanted to get as strong as possible before treatment began. Specifically, I say:
My number one priority pre-surgery is biking. That is, back when I thought I might have cancer (after my family doc appointment) the one thing I decided was that I would train so that I was in the best physical shape possible before surgery/chemo. I want to make sure I’m going into this as strong as possible. For me this means allocating 2-3 hour a day (or more) for biking.
As time progressed, I added hiking to my repertoire of exercise. I especially found exercising in nature as a way to feel both physically and mentally better. I highlight the effect of hiking in a grove of ancient redwood trees:
I find peace in nature, so today we spent some time communing with nature. We went for a walk in the Redwoods up at Big Basin Redwoods State park. We walked for 9km, that’s a record for me. Big Basin Redwoods is perhaps one of my favourite places. The trees are literally 1000s of years old. There is a peace when you are walking and touching these ancient trees – some with battle scars from fires long past. They are survivors.
Unfortunately, the side effects of chemotherapy caught up to me as I had mouth sores that made it impossible for me to effectively hydrate, which in turn curtailed my ability to exercise (Not talking = not blogging, August 30, 2014). After surgery, I returned to regular exercise as a way to recover:
Recovery is still a long road. My hematocrit tanked again (lower than ever). I find myself easily out of breath while walking or climbing a single flight of stairs. My incisions are healing well. I still have a couple of drains which I’ll probably have until next Monday as they are still producing a fair amount of fluid. For the next week, we shall take one step at a time, trying to increase my walking distance and awaiting the day when I can get back on the bike.
Further, post-surgery I was thankful for all the time I spent exercising during chemotherapy, because “when I took my first steps, my legs were strong. It made a huge difference to how quickly I was able to move, and how quickly I’ve been able to walk.” (A small cup of coffee, January 2, 2014).
Social Networking
Initially, I was very hesitant about joining any breast cancer communities. It was my husband who pushed me to attend my first support group meeting, only a few days after my diagnosis. In Support group (June 22, 2014), I express how attending the support group helped me learn to talk about my cancer. I had to say it out loud. It also gave me a space to talk about breast cancer with others who understood what I was going through.
Further, in Joining the cancer blogsphere (July 6, 2014), I expressed my hesitation in joining the breast cancer blogosphere:
I have strong online relationships. I am part of several online communities where I find strength and much needed support. But, to join a cancer community means to admit that I have cancer – but there is more to it than that – it is the fear of joining a community and then losing people in that community. I’m OK with admitting I have cancer, but I’m not OK with admitting that it is something that might one day kill me. I’m afraid that if I develop solid friendships with others who have cancer, that I’ll lose them. I don’t want to have to deal with the death of a good friend – and so, I hesitate. I hesitate to reach out too much to others who are also going through this experience – not because I don’t want to meet these people or get to know them – just that I don’t want to get to know them and then lose them.
Despite my hesitance to reach out to new support communities, my posts show that I did reach out to my pre-existing social networks for support. For example, when I found that I needed support to overcome inertia and side effects in order to exercise, I called on friends to help keep me accountable and help me get off the couch using a personal Facebook exercise support group (Significance of dates and getting ready for chemo, June 26, 2014).
Further, the importance of social networking as a coping mechanism was suggested when I blogged about the role of social media in my process of gathering information about breast cancer and treatment options. In Social media and patient engagement (October 29, 2014), I outline what type of information I gathered from social media:
I have been reflecting on social media and the type of information I get from social media. I use social media to get a sense of the ‘lived experience’ of a given treatment. When I reach out and ask, I receive experiences from others as well as a boat load of advice. This information is often very useful in helping me better gauge what to expect, but also in helping me ask questions of my healthcare team.
In addition to using my social network for outside support, my blog also highlighted the importance of having a caregiver to provide support when I was not able to make decisions for myself. The impacts of cancer and chemotherapy on my mental capacity meant that I could no longer troubleshoot when unexpected events occurred. My husband, Scott, was my rock and was there to ensure continuity of care. After my first surgery, where he could stay the night in my hospital room which “turned out to be very useful, as several times I benefitted from having a patient advocate (things like helping when I needed to use the toilet). It also meant that he was here for most of the doctor and nurse visits.” (An update from the hospital, November 20, 2014). Further, caregiver support was highlighted when I blogged about the challenges of returning home after my second surgery:
When we got home one of the biggest challenges was figuring out all the medications and a schedule that allows us to create an efficient process. I can now better appreciate why it felt like the nurses were giving me various pills on an almost hourly basis. Someone asked how many? I’m at 17 different meds, with 11 different dose times. The goal in setting up a schedule was to optimize pain medications and reduce the number of times in the day I’m taking drugs, while still respecting various drug interactions. This isn’t something that is easily done by the pharmacy, as the pharmacy doesn’t deal with all the over-the-counter meds that are also prescribed (e.g. I’m prescribed certain vitamins which aren’t provided by the pharmacy).
Seeking Control
Initially one of the ways I exhibited the theme seeking control was through intentionally finding ways to have fun. This became an explicit activity. I knew that if I didn’t find ways to have fun then treatment would be very difficult: “One of the things that causes that natural high for me is sailing. So, we are looking for ways to go sailing regularly. However, sailing can be very physically demanding, which will likely be a challenge. This Saturday, we are headed up to the city to go sailing on a 2003 America’s Cup boat.” (Priorities, June 18, 2014).
In addition to intentional fun, I also had to explicitly give myself permission to do things. Initially, it was giving myself permission to nap (I had to give myself permission to nap, July 9, 2014). As the idea of surgery approached “I have given myself permission to go into surgery kicking and screaming. I’m OK with not being calm and collected when I get rolled into surgery. It is natural to not want to deal with it.” (I’m scared, September 17, 2014).
After I began chemotherapy treatment, one of the ways I attempted to regain a sense of control was to shave my head prior to losing all my hair. I explain this decision:
If you haven’t done a chemo that causes hair loss you may not understand this idea of proactively shaving your head. There are a couple of reasons for it. The practical reason is that hair falling out in clumps is a pain. The second, more important one, is an exercise in control. If I’m going to lose my hair, then I am going to control when it happens. Control is a huge issue with cancer, as it is one of the things you lose. You lose a lot of control over how your body is growing, how it reacts, and the various schedules of appointments. When you have an opportunity to take control and do something on your own terms, it can be important for some people to take control.
Further, to help plan for chemotherapy side effects, I created a chart of my symptoms, see Image 1, which I used to help predict when I was going to experience the different side effects in future chemotherapy cycles. I also used the chart to determine which steps I should take to proactively reduce the impact of the side effects (Mouth sores & first cycle symptoms, July 20, 2014).
Image 1: Chart indicating the timeline of anticipated chemotherapy side effects.
Perhaps one of the more pragmatic attempts at seeking control was through planning. Unfortunately, the unpredictable nature of chemotherapy treatment meant that some of the plans I had originally made, specifically my original plans for a trip to Hawaii, would no longer work. Additional planning was required regarding the new treatment schedule:
I’m actually of quite mixed emotions. This plan works for me – it lets me still get in a trip to Hawaii before the first surgery, and a trip to visit my parents before the second surgery. We ran through the schedules last night, and it even looks like my friends from Nova Scotia can still join us in Hawaii (yay). The extra chemo gets me that much closer to finishing the protocol (which calls for 12 sessions of Taxol – in the end I’ll have 9 sessions). Part of me doesn’t want the extra two chemo sessions – I’d just like to stop chemo and go on with the surgery, but another part says – what if those extra two are the difference between beating this thing and not? Will those two extra sessions be extra insurance against recurrence? Metastasis? Of course, we don’t know. We have no way of knowing whether or not a couple more sessions of chemo will make any difference what so ever. But to align with the surgery schedules, it is best that I am in chemo right up until three weeks before surgery. And then I get four weeks between the first surgery and the second surgery. I’m happy for a little extra time to ensure that I’ve healed.”
Finally, the post-surgery posts in seeking control relate to advocating for myself during interactions with the healthcare system. Specifically, I wrote about negotiating with a resident regarding a surgical side effect, and my unwillingness (non-compliance) to take her recommendation:
Sensing my non-compliance, she asked if I was okay with the plan. I said “no, how about we watch and wait? — because I am passing some urine, I’m not completely blocked — it is just taking time and not flowing properly”. I don’t completely trust the resident’s opinion. I want to hear it from someone with more experience.
Summary
One of the important aspects of health-related self-efficacy around cancer care is the need for the patient to develop coping mechanism (Papadakos, 2017). In my theme analysis of the category Developing coping mechanisms, I show that I continually developed coping mechanisms throughout treatment. Under the category of Developing coping mechanisms, I constructed four themes (1) blogging, (2) exercise, (3) social networking, and (4) seeking control. Blogging was initially a way in which to help me process and share my treatment decisions. Later, blogging became a way of exercising my mind, where physical exercise provided a way for me to feel physically and mentally better. Throughout the study period, I found support in both face-to-face and online social networks. The theme social networks also included support that I received from my husband and primary caregiver. Finally, I blogged about the ways in which I sought control, including intentionally planning fun activities and travel. Control seeking was also expressed through self-advocacy.
My analysis of the category Developing coping mechanisms showed that I continually developed coping mechanisms throughout treatments. Although each individual chooses to cope in different ways (Al-Azri, Al-Awisi, & Al-Moundhri, 2009), blogs such as mine provide a great resource for discovering what coping mechanisms might be useful. A practice that I developed through my experience was to develop coping mechanisms such as blogging, social networking, exercising, and seeking control. Patients experiencing critical or chronic illness have a need to develop coping mechanisms in order to learn how to live with illness.
References
Al‐Azri, M., Al‐Awisi, H., & Al‐Moundhri, M. (2009). Coping with a diagnosis of breast cancer‐literature review and implications for developing countries. The breast journal, 15(6), 615-622.
Papadakos, J. K. (2017). The Association of Health Literacy and Self-Efficacy to Cancer Chemotherapy Self-Management Behaviours and Health Service Utilization. Doctor of Philosophy.
Are you a patient? Do these coping mechanisms align with your experience? What other types of coping mechanisms did you develop?
I had originally planned on waiting until December 17 to release my book – that would be the 8th anniversary of the surgery to remove the last of the known cancer from my body. However, when I had the paperback ready, Amazon did not let me publish it on a future date. That meant that the paperback version was ready but the eBook was being held back. And so, I have now released the eBook, Kindle unlimited, and Paperback versions of “Never Knew I Wanted to be a Breast Cancer Survivor”. I’ve ordered some author copies for myself, but they have not arrived yet – however, I have heard from friends that their copies have arrived.
I hope you enjoy the book.
When I was working on it, I was working on a PhD. That involved analyzing the blog posts for key themes. The themes helped me choose which of the blog posts made their way into the book. The themes I identified are:
Developing coping mechanisms
Navigating the healthcare system
Learning about the disease
Understanding side effects
Advocating
Exploring body image
Making decisions
Negotiating identity
I came to the conclusion that these themes aligned with patient health literacies that I developed throughout my treatment experience.
Patient Health Literacies – (c) 2020 Rebecca J. Hogue
If you are reading the book, can you see these themes? Do you see any other themes in the book?
It is hard to believe, but true – The eBook version of first book is now available for pre-order on Amazon. The print version is coming soon – I’m just waiting on a proof before I release it. It has been quite the journey getting this far.
The book started out as this blog.
It was then an important chapter in my dissertation, but never got published because I walked away from the PhD.
Now it is an eBook and will soon also have a print version. This is what I’ve really wanted all along. The PhD helped me to analyze the original posts for themes, and pull out the important stories from the blog, but it was the sharing of the story that is what I really wanted to do.
The book tells my story from diagnosis until active treatment. My next project (and hopefully book) will be the first year after treatment. That time was in many ways so much harder for me than the year of treatment. It took a lot for me to figure out how to cope with the anxiety.
What the book doesn’t include are the analyses that I did around the blog and the information I gleaned from the process. I will start to blog about these insights – because I think it is valuable information – and I also think is a good quick way to get it out. I guess I could create a companion guide for health educators that includes the insights from the dissertation. That is an interesting idea. I’m not sure how much demand there would be for it!
I chose December 17 as the release date for the eBook – but I might change that. December 17 is my “cancerversary” – in that it is the day that I choose to acknowledge my experience and recognize it as the day the last known cancer was removed from my body. However, the print version of the book will likely be available for order sooner.
I never thought I’d want to be a breast cancer survivor brings you into Becky’s world as a young breast cancer survivor. Written initially as a blog, Becky shares her experiences with treatment starting the day after she first heard the words “you have breast cancer”. Throughout her treatment, she explains her thought processes as she grapples with life altering treatment decisions: which chemotherapy regime? to reconstruct or not reconstruct?
Humorous at times, serious at times, this memoire will have you laughing and crying as Becky shares her feelings but also what she is learning as she discovers what it means to be a breast cancer survivor.